How long should a dental implant be?
This article analyzes the nuances of choosing the optimal length and diameter of a dental implant. There is evidence that the upper 8-12mm of the root implant actually works. There are even results for modeling that say that only 5-6mm of an implant are maximally loaded, and the part that is deeper is not exactly useless, but in many cases is unnecessary. We determine when a long implant is necessary, and when it can cause harm and risk losing the prosthesis. Whereas, a short one (about 10mm) will never create such problems.
The length of the implant that is considered to be sufficient in everyday practice
It is not that easy to define the sufficient length of the implant as there is a lot of empirical (unproven) experience in the field of dental prosthetics. This is when each dentist relies on his own practice and the results he obtained. For instance, a dentist put dental implants of a certain length (for example, 12-14mm) during 10-12 years, and if most of them are still in place, then the choice was right.
It is difficult to argue with this fact, but there are studies published in 2011, albeit in a mathematical journal in the context of methods for mathematical modeling of the distribution of loads in a heterogeneous medium. However, dentures were chosen as objects of modeling. This allowed us to work out what is really happening with the implant, namely, how and in which part of the bone the loads are distributed and which part of the implant is most loaded.
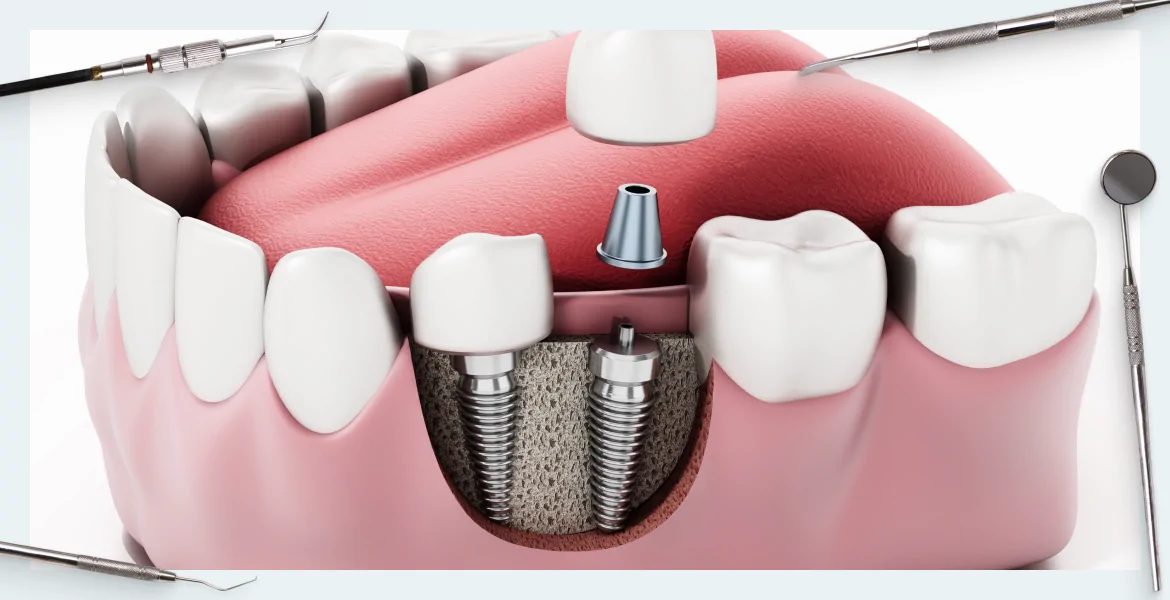
Modeling of loads was carried out using photoelastic models of the jaw bones.

Both axial and lateral loads were simulated and applied at an angle of 30 degrees. The modeling of the load corresponds to the lingual – buccal load on the tooth when chewing.
As a result, it was possible to collect data and analyze which part of the implant works, to be specific, it is exposed to the maximum load in the vertical, and especially the lateral plane. Bones of different strength and shape were modeled in combination with root implants of different lengths and diameters.
As a result, a 12mm long implant with a 4mm platform was recognized as standard and sufficient for more than 85% of clinical cases for installation in the native bone (completely healed bone-carrier).
In addition, as confirmed by the number of sales, dentists most often buy dental implants with a length of 10, 11 and 12mm, and sets of abutments for them.

Moreover, it has been found that the diameter of the implant has a great influence on the occurrence of over-stresses, in other words, the wider the implant is, the more secure it is, which means it can be shorter. After all, the load is distributed more evenly with a wide implant, because the circumference and the area of external contact with the native bone are larger.
What is bicortical anchorage of the dental implant?
What is it for?
The question may arise why it was only in recent years that an implant with a length of 10-12mm and a platform width of 4-4.5mm began to be called standard, and why longer root implants were previously installed. In fact, everything is simple, at the dawn of modern methods of prosthetics, there weren’t powerful computers and methods for constructing mathematical models of load distribution.
In the days of Branemark, no one knew what length would be appropriate. However, that’s not to say that they put an implant by eye with a margin, so that after osteo-integration it was held securely. In those days the theory of bicortical integration was widespread. The cortical layer of the bone is the hardest layer. Therefore, for example, when installing an implant in the upper jaw, the implant passes through the first cortical layer of the alveolar bone, and if the length permits, it passes closer to the maxillary sinuses and is re-anchored in the cortical layer of the nasal cavity. This is where the term bicortical anchorage comes from. For a long time it was considered that this method is better and more reliable than fixing the implant only in the jaw.
Moreover, as it stands today, this point of view is considered correct among many GR dentists.
However, this theoretical model was refuted by Branemark himself, or to be more accurate by a group of Swedish researchers co-authored with Branemark.

They collected and analyzed data from long-term (10-15 years) observations of implants installed using bicortical and monocortical anchorage, see the illustration below. 100 dental implants installed using both methods were observed and studied.

The results were surprising. The number of complications and cases of loss of implants was higher where bicortical anchorage was used. The number of implant loss cases was four times higher compared to monocortical anchorage. Moreover, 87% of cases of prostheses loss were associated with a fracture of the implant. It turned out that an implant so securely anchored on both sides experiences high overstresses at bends and does not withstand them. In contrast, in a monocorticaly anchored implant, lateral loads are compensated and dissipated in the softer (cancellous) part of the bone. After all, the alveolar bone is alive. In addition, it cannot be considered as a solid structure like brick or concrete, into which you need to drive a dowel. It can bend to respond to the load applied to the denture.
It goes without saying that no prosthesis can compare with a living tooth, but a well-engrafted implant can also slightly sag and deviate in the lateral plane and return back without negative consequences. Furthermore, with regular significant loads on the implant, corticalization of the surrounding bone occurs. This means that the bone tissue becomes denser and stronger around the part of the implant that was in the cancellous part. While, a long implant anchored on both sides experiences significant loads and often does not withstand. This fact is confirmed by the results of this study.
As a result, the theoretical benefits of bicortical anchorage were not confirmed; on the contrary, it turned out that this method of anchorage is unnecessary and in many cases even harmful.
What influences the choice of implant length?
If, as it stands today, the standard length of the implant is 8-12mm with a width of 4mm, then first you first need to check if there are any contraindications for a particular case. Namely:
- Poor condition of the alveolar ridge. It is not always possible to install a root implant with a diameter of 4-4.5mm. If the ridge is thinned. You may need to choose a thin (2.5mm or 3mm) implant, but it shall be longer.
- Place and method of installing a denture. When it comes to the cosmetic area, we mean the incisors located in the upper jaw, you also need to choose implants of a smaller diameter, but longer, especially if the installation of an implant and a temporary crown is expected on the same day as the removal of the problem tooth. After all, in this case, we will not have several months for engraftment and osteo-integration when the implant is closed with a healing abutment and is not subjected to stress. Therefore, a longer abutment should be used. We will analyze this specific case in more detail below.
What part of the implant does actually “work” in the bone?
If, today, the standard length of the implant is considered to be 8-12mm, then you can often find information that only the upper 5-6mm are really loaded and work. This statement is also well-grounded. There is a study dated 2010.

Research was carried out using photoelastic models and mathematical modeling. A range of implants of various platform lengths and widths was used as a base. In addition, researchers used implants with different platform widths, but with the same body of the root implant.
The modeling process allowed us to review how the load is distributed from all possible directions including extreme angles and forces.
Dental implants of different diameters were installed, namely, from 2.mm to 5mm with all intermediate options: 3.5; 3.75; 4.0; 4.5mm, etc. It was possible to combine them with different platform options. For example, the implant body is 2.5mm and the platform is 3.75mm or 4.0mm or even 5mm. Options for the length of the implant body ranged from 8 to 15mm.
As for the load, an axial (direct load) and a lateral load were simulated at an angle of 30 degrees, same as what occurs with lateral movements of the jaw.
The relationship between the occurrence of point loads and the implant diameter was confirmed.
If we increase the diameter of the implant body, let’s say from 3 to 5mm, we can reduce the point load on the alveolar bone by 30%. It was also confirmed that the main load is borne by the part of the implant located apically (higher, not deeper), namely, 8.5mm in the alveolar bone. To be more accurate, the maximum load is borne by the first six coils (an average pitch of 0.85-1mm), and then the workload decreases noticeably and almost disappears after 12-13mm. Six coils with a pitch of 0.85-1mm ensure those 5-6mm.
When and why are long implants needed?
There is only one situation when long implants are needed. This happens when the installation of an implant and a temporary crown is carried out on the same day with the extraction of a tooth, especially when it comes to the cosmetic area (front, especially upper teeth). We load the restored tooth immediately. Even if the crown is made so that it does not come into direct contact, only an insignificant part of the load will be removed.
To obtain the greatest possible primary stability, the body of the threaded rod must be as deep as possible. And this is
the only case when you need a length of 14-16mm or more (up to 18mm).
This is despite the fact that the roots of the incisors and primals are rarely longer than 9-12mm, which seems to correspond to the previously mentioned standard for dental implants of 12mm.
The picture below shows that if a 12mm implant is installed, so that the implant substructure is located just below the ridge of the alveolar bone, then the main load will be borne by the last 4mm of the threaded rod. Thus, the load through the screw on the abutment and the crown will act as a lever. Because of this, the risk of losing the implant increases dramatically. Therefore, in the future, the specialist will face an even greater bone deficit to carry out the repeated implantation.
The 4.0mm that bears load is only a third part of the total length and that is not sufficient. The situation is better in the second picture.

An implant of the same diameter (3.75mm), but 15mm long, was used here. 5.5mm ensures the primary stability in this particular case. This is significantly better, although it is still 5.5mm, in other words, it’s only about a third of the total dental implant length. Finally, the last picture shows an implant 18mm long.

Such an implant will need to be installed at a slightly different angle. This creates some difficulties, you may have to order a custom or cast abutment, but we have already anchored 9mm for primary stability. So, this is already half of the total length of the abutment. This is a very good result.
After all, as you know, at the stage of engraftment, first a partial loss of primary stability occurs and then secondary stability is acquired as a result of osteo-integration. Therefore, if only 4mm or even 5mm is involved, then the risk of losing the implant will be too high.
That is just where we face the problem because most manufacturers do not have dental implants longer than 14mm. That is why you have to look for them, order separately and keep a stock at the clinic.
We hope the material of this article was useful to you.







