Which is better: single implants or bonded bridges on implants




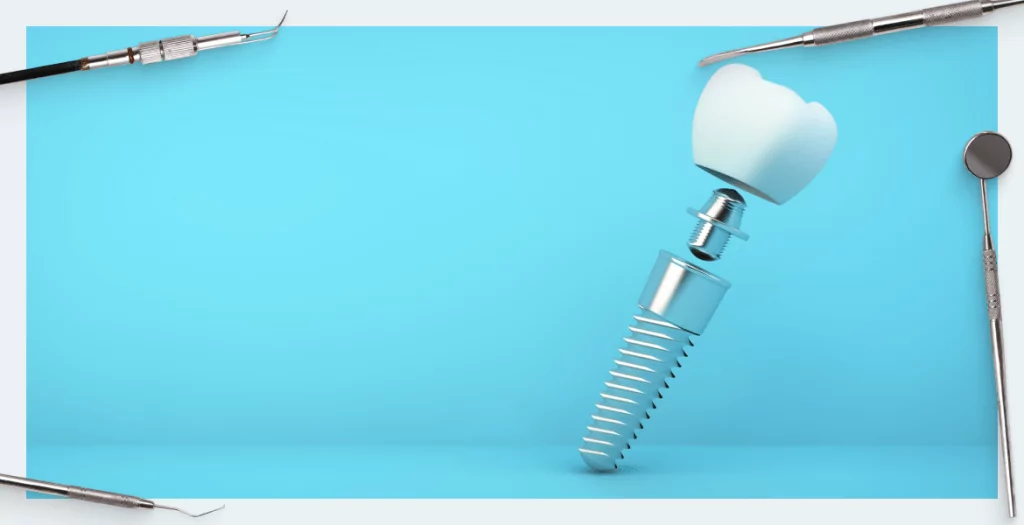
Which is better: splinting or single implants? We are talking about the mechanical binding of several prostheses located next to each other, see the picture below. This is a matter of pure mechanics and does not affect the implantation technology in any way. At first glance, it is logical that the bonded structure is stronger and the load on the bone is distributed more evenly, see the picture below. The picture shows that the abutments for the implants remain individual, and only the crowns are connected. However, the experts are not interested in the general logic; they are interested in the exact data obtained as a result of research. After all, there are traps and pitfalls everywhere, and we need hard facts, not assumptio
Advantages of splinted implants on individual implants and abutments
As proven by research and dentists’ experience, there is no difference between the techniques in the stage of engraftment and formation of the gums with healing caps. However, when ordering crowns for the restoration of the dentition, you need to make a decision whether to tie them or to make them individual.
It is better to combine implants because:
- The splinted system relieves the point load from abutments, screws and other elements of the prosthesis.
- The connected dental bridge also reduces the point load on the jaw bone, which is clearly visible in the picture, where the areas of increased load on a single implant are highlighted in red.

For the purpose of carrying out research, models with pressure sensors were manufactured, on which the restoration of the dentition was imitated both with single prostheses and with coupled ones. Then the pattern was exposed to loads on special equipment to take a diagram of the distribution of loads both on the elements of the prostheses (abutments, screws etc.) and on the jawbone, see the picture below.
Since the bone is a vital structure that can compensate for loads through elasticity and gradual compaction of the structure in response to regular loads, the “red zone” in the diagram above is not a critical obstacle to single implantation. - There is no significant difference when using single or linked implants. However, the risk of losing implants after engraftment is higher in the case of installing single prostheses because abutments for dental implants work like a lever and transfer the load to the bone that surrounds the denture. The difference with linked implants is not very large, but the likelihood of losing an implant is clearly associated with the single-placement technique.
This is confirmed by research results and meta-analysis. There are only a few such studies, but they do exist. It is very difficult to make a qualitative review, as in any research related to orthopedics. After all, statistics should be objective, and the sample should be randomized (randomly, blind). The main difficulty, as always, is the human factor. It relates to both, on the part of patients and on the part of specialists. After all, the more experienced and highly-trained the specialist is, the better his statistics are, no matter what methods he uses. In addition, a lot depends on the patient, because people often do not follow the recommendations for caring for their dentures, and there are also frequent problems with basic oral hygiene. The lifespan of prosthesis is highly dependent on both the implantation technique and the patient’s lifestyle. - There is an interesting study that used a high-precision camera that recorded the degree of divergence of linked and single implants under load in a special machine. The study compared how single and splinted implants behave with and without distal contact. The results showed that significant overloads are observed in the collumn of the prosthesis in a single implant in the absence of distal contact. This means that the bonding of implant crowns also works better in situations of partial restoration in the absence of the next tooth.


We would like to present the conclusions of a complete review, which includes biological and technical complications in different methods of restoration of the dentition on implants.
 According to the results, splinting of dental implants is recommended for the following cases:
According to the results, splinting of dental implants is recommended for the following cases:
- availability of bruxism (teeth grinding during sleep);
- bone problems, weakening of bone tissue (porous bone), etc.;
- if only thin and short implants can be installed.
Installation of single implants is recommended for the following cases:
- three or more consecutive implants – associated with the quality of the fit, but we will analyze the nuances of the passive fit below;
- if it is difficult for the patient to follow the rules of oral hygiene (old age, dementia, mental disorders); but the difference in caring for single and coupled dentures is insignificant.
Disadvantages of bonded implants
The problem with passive fit of the restoration is that it is always more difficult to perfectly position the combined structure on the pins. This becomes especially obvious when installing extended structures, such as bridges for restoration of the dentition with complete or almost complete edentulism. In these cases, some segmentation is recommended with the installation of unlinked blocks of 3-4 teeth. It would seem that this is a serious argument against splinting. However, there are research results from Dr. Guichet and his colleagues University of California.

They did not just compare how splinted and non-splinted implants behave under load. They also compared how single implants behave taking into consideration the difference in the degree of contact with each other. Three crowns were installed on three individual abutments. There were five contact/gap options between the crowns ranging from zero (where there is no contact at all, the crowns do not touch under any circumstances) to perfect contact, where the gap is minimal, but this is not yet a monolithic structure.

- perfect contact – the gap does not exceed 8 microns, a carbon copy 8 microns thick passes and does not break;
- light contact – 10 microns have been added to the previous gap; the carbon copy will no longer pass; the load between the crowns increases;
- middle contact is perfect contact plus of 50 microns;
- tight contact is perfect contact plus 90 microns.
The results showed that the best passive fit is observed for the zero contact and the perfect contact option. At this stage, the assumption that individual prostheses are better for a good passive fit seems to be confirmed.
In reality, it is almost impossible to achieve perfect contact between the crowns. When the internal stress from the contact between the crowns is added to the axial and lateral loads, this creates additional stress on the columns of the screws and abutments. Whereas the splinted structure is a monolithic element and does not create such problems, but on the contrary effectively relieves the supporting elements of the implants, although the passivity of fit in this case is somewhat worse. Thus, this disadvantage of bonded crowns turns into a virtue.
Single and Bonded Implants – Comparison Chart
The color of the cell illustrates how reliable and problem-free the implant is. Green is good, pale green is good, but not as good as the alternative option. Yellow is also good, but there is a noticeable risk of complications.
| Characteristics | Splinted bridge | Single implantation |
| Durability (risk of losing the implant) | High probability of survival (engraftment) and service for 5 or more years. | Commensurate with the bonded, high probability of survival for 5 years or more. But there is a slight but clear trend towards a greater risk of losing a single implant |
| Loss of marginal bone | Moderate within 0.7-0.9mm | Moderate within 0.7-0.9mm |
| Peak load distribution | Uniform point overloads are practically not observed | There are clearly defined point overloads both on the mechanical parts (screw and abutment) and on the vital bone |
| Risk of screw loosening and loosening of crowns | Minimal | Much more common due to high point overloads |
| Ceramic chipping risk | For the restoration of the dentition;
does not differ from the single |
For the restoration of the dentition; does not differ from the bonded one |
| Patient quality of life | High, the patient does not feel any problems in daily life | High, the patient does not feel any problems in daily life, but the risk of technical complications is higher |
| Any difficulties for the patient to take care of his oral hygiene | Care and cleaning is the same as for all other denture systems. But it also depends on the location and physical implementation of the implant. It is often, but not always, more difficult to take care of a splinted restoration. Some experts point out the impossibility of flossing. Though, this method is not recommended for dentures, due to the high risk of injury to the gums. A denture is not a living tooth and floss injuries can lead to serious complications. | Care and cleaning is the same as for all other denture systems. |
Based on the number of green cells and the degree of their coloration, it can be concluded that the binding of implants is recommended in most cases. Although, there are always contraindications and advice from a highly-specialized doctor is always needed.
We hope the material in this article was useful to you.